

Take home message
- The meaning about milk fat consumption in relation to cardiovascular disease and all-mortality has changed dramatically; the negative correlation conjured up by Ancel Keys in the 1950-60s about animal fat consumption is not true.
- What is new, however, is that it does matter from which milk product the milk fat is (mainly) absorbed. Consumption of whole milk picks up more unfavourably, unlike fermented dairy (yoghurt, kefir, cheese).
Whole milk or not?
There is regular ambiguity again, whether milk consumption contributes to health and mortality. A long-term study of Swedish women who took part in annual mammography screening also looked at the relationship with their diet. Earlier, it became clear, that the mortality risk is different between women drinking plain milk and those taking fermented milk products (Acidophilus milk) or cheese. New, additional research (Michäelsson and Byberg, 2020) looked at whether there were differences between different fat levels of milk consumed (0.5%, 1.5% and 3.0% fat). A large group of women was included in the study (n=61,400), which gave the opportunity to compare different groups. So, there are two questions: (1) what is the impact of the fat content of milk consumed? And (2) what are the consequences of an increasing amount of milk consumption?
Swedish women all drink roughly the same type of shop milk – pasteurised and homogenised. There is hardly any UHT milk or raw milk consumption. The age of the women at baseline is around 54-55 years and they have a BMI close to 25. Over the course of the study (23 years), 22,500 women died, regardless of cause. This is called the ‘all-cause mortality’ and has the advantage, that you don’t need a doctor’s opinion or an autopsy, because you do not bother about the cause of death. Because of the large group of women in the study, groups were built that consistently drank a certain type of milk (e.g. always milk with 1.5% fat). However, all women also took on average half a glass of sour dairy and some cheese/day. For statistical evaluation, the relative risk (hazard ratio) of each group is compared to a control. The control is mostle the group with the lowest consumption (here: less than 200ml/day. On average, the real amount of consumption was 17ml of milk/day (which is 1 glass every 2 weeks). Figure 1 shows three lines, each representing a fat content group (0.5%, 1.5% and 3.0% fat).
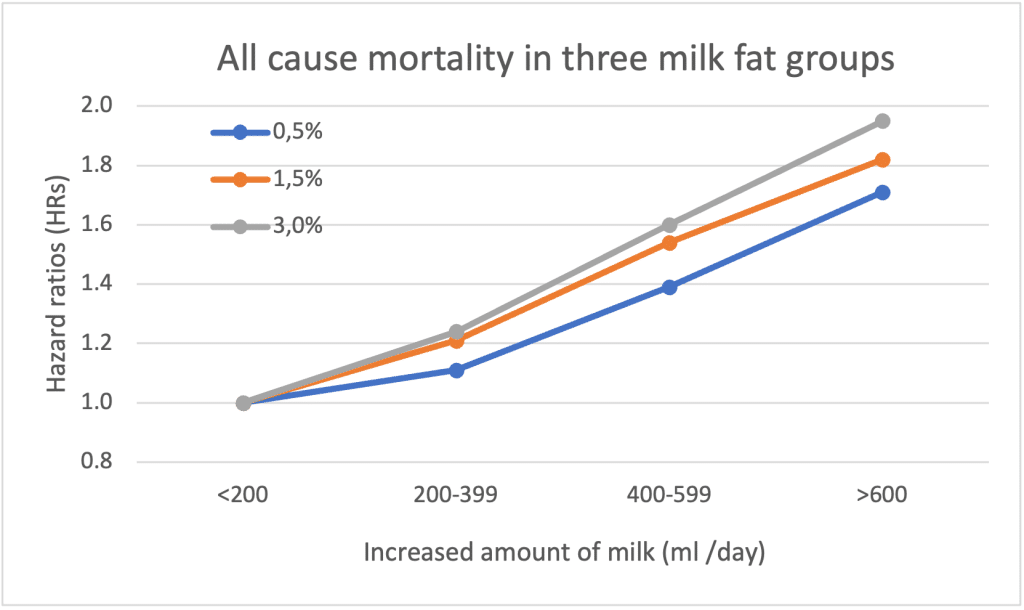
As in a previous study (Michäelsson et al., 2014), there is a higher risk to die when women consume more plain milk; in all three levels of milk fat there is an increased mortality. Interestingly, however, the risk varies between the fat contents of the milk, and the more milk fat you consume (3.0% fat), the higher the risk of death. So, there is clearly a negative effect of the higher milk fat intake from whole milk. The increased risk to die is almost 2x higher (HR=1.95) in the highest consumption class of milk drinkers of whole milk (3.0% fat) (on average 700 ml of milk/day), compared with the low milk drinkers.
Biomarkers for milk fat intake
Another group of Swedish researchers took a different marker for milk and dairy consumption (Trieu et al., 2021). They used the blood levels of odd saturated fatty acids to calculate the dairy intake. Pentadecanoic acid (C15:0) was measured in people over 60 years of age and correlated with cardiovascular disease (CVD) mortality and total mortality. In contrats to the study above, the risk for CVD is lowest in the group with the highest C15:0; this means the more milk fat consumed, the lower the risk of CVD mortality. The correlation was different for total mortality, and the relationship was not linear, but showed a U-shape. The lowest overall mortality is found in the group with the average C15:0 blood value. This implies, that both less and above average milk fat intake is at risk. The results of the two Swedish studies seem to contradict each other. However, the biomarker C15:0 does not say anything about the type of dairy eaten, it is rather a general plea, that fat from milk products is not bad per se. Trieu do indicate, however, that differentiation between products is necessary, in a way that was implemented in Michaëlsson’s study.
Too high for which type of (milk) fat?
There are several studies that address the difference in mortality or cardiovascular disease in relation to the type of milk product consumed. Australian researchers (Xu et al., 2022) took the group of people diagnosed with cardiovascular disease. They distinguished six different disease states, but the results below apply to the group. The people involved were already older, close to 70 years old. There are four groups of milk drinkers: whole milk, semi-skimmed milk and skimmed milk; in comparison to a group that drank soy milk. Furthermore, there are men as well as women. The whole milk drinkers die the fastest, like Michäelsson’s results above. When corrected for background differences between the groups (gender, BMI, alcohol consumption, etc), significant effects remain between whole and semi-skimmed milk drinkers. Differences between whole milk and skimmed (0% fat) milk are also found, but only for males. There is a risk reduction of about 30 or 40% for the 2% and 0% fat milk (HRadj = 0.69, P=0.004 and HRadj = 0.59, P=0.016 for men and women, respectively).
Joris Driepinter: exit?
Joris Driepinter was the Dutch advertisement to increase milk consumption in the 1960s-1970s. The slogan was “drink at least 3 glasses of milk per day”, of course for reason of strength and health. Apart from the question, if the slogan was much more an industrial push for more milk consumption rather than a valid health claim; times have changed, dietary habits are different, the amount of food available is different and obesity is more likely to increase. It may very well be, that milk fat quality changed overtime, because our cows were fed differently 50Y ago and give nowadays much more milk. It could also be, that fresh, whole milk is mainly meant for the young child following the breast milk phase of its own mum. Further whole milk at the start of the 20th century had around 2% fat, whole milk now above 4.5% fat.
At higher age, fermented milk products are more appropriate than unfermented milk. Possibly, because it better nourishes the gut and supports its functioning. What also might be interesting, is the consumption of raw milk rather than processed shop milk. All studies mentioned here apply to pasteurised milk. In contrast, in a survey of US consumers of raw milk (Baars et al., 2019), people indicate that they very much benefit from raw, whole milk. The focus of the raw milk study was not on mortality, but perceived health and immunity, gut and skin health.
Literature
- Baars, T., Berge, A. C., Garssen, J., & Verster, J. C. (2019). Effect of raw milk consumption on perceived health, mood and immune functioning among US adults with a poor and normal health: A retrospective questionnaire-based study. Complementary therapies in medicine, 47, 102196.
- Michaëlsson, K., & Byberg, L. (2020). Mixing of apples and oranges in milk research: A cohort analysis of non-fermented milk intake and all-cause mortality. Nutrients, 12(5), 1393.
- Michaëlsson, K., Wolk, A., Langenskiöld, S., Basu, S., Lemming, E. W., Melhus, H., & Byberg, L. (2014). Milk intake and risk of mortality and fractures in women and men: cohort studies. Bmj, 349.
- Trieu, K., Bhat, S., Dai, Z., Leander, K., Gigante, B., Qian, F., … & Marklund, M. (2021). Biomarkers of dairy fat intake, incident cardiovascular disease, and all-cause mortality: A cohort study, systematic review, and meta-analysis. PLoS medicine, 18(9), e1003763.


